ACE Inhibitors and ARBs: Understanding Interactions and Cross-Reactivity Risks
ACE Inhibitor & ARB Interaction Checker
This tool helps you understand the risks of taking ACE inhibitors and ARBs together. Based on major studies like ONTARGET and VA NEPHRON-D, combining these drugs increases serious risks without improving outcomes.
Select your medications above to see interaction risks.
When you're managing high blood pressure, heart failure, or kidney disease, your doctor might prescribe an ACE inhibitor or an ARB. These drugs are common, effective, and often lifesaving. But what happens when you take both? Or switch from one to the other? The answer isn’t as simple as it seems.
How ACE Inhibitors and ARBs Work
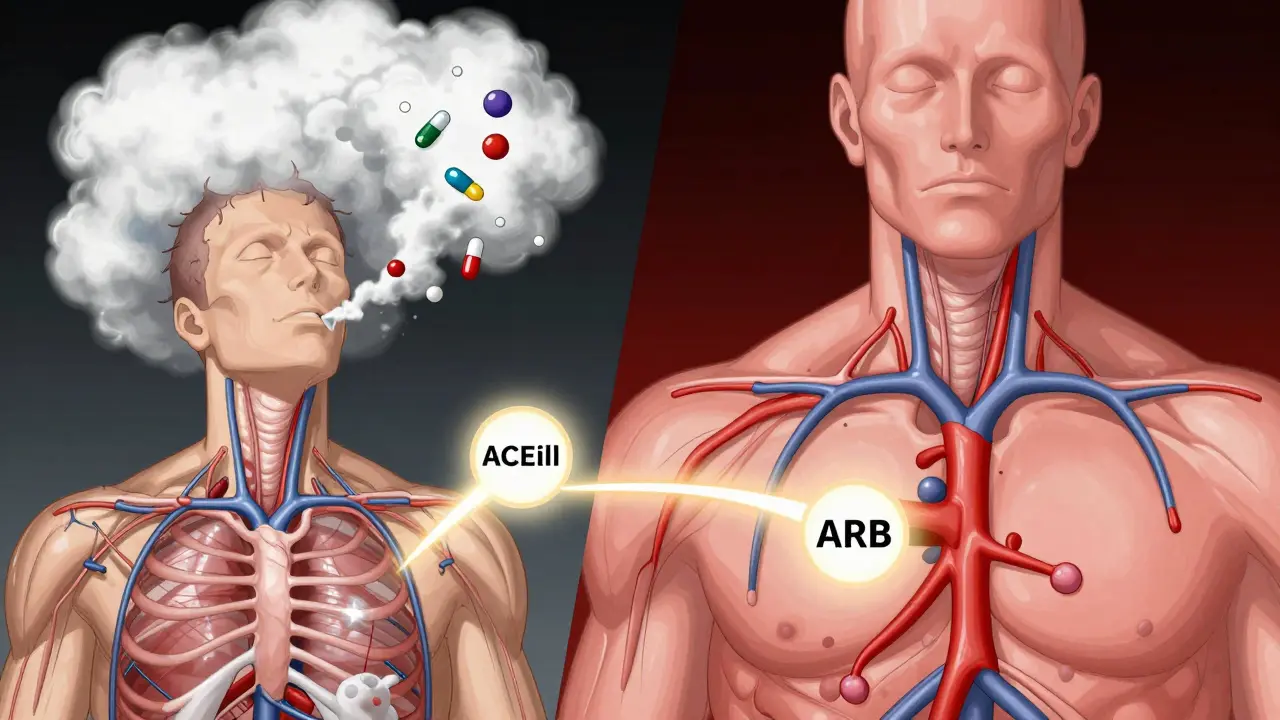
Both ACE inhibitors and ARBs target the same system in your body-the renin-angiotensin system (RAS)-but they do it in different ways. ACE inhibitors, like lisinopril and enalapril, stop your body from making angiotensin II, a chemical that narrows blood vessels and raises blood pressure. By blocking the enzyme that turns angiotensin I into angiotensin II, these drugs help relax arteries and reduce fluid buildup.
ARBs, such as losartan and valsartan, work downstream. Instead of stopping angiotensin II from being made, they block its receptors. This means angiotensin II is still present, but it can’t bind to the receptors that cause blood vessels to tighten. This difference might sound small, but it leads to real-world differences in side effects and safety.
One key point: ACE inhibitors cause bradykinin to build up in your system. That’s why about 1 in 10 people on these drugs get a dry, persistent cough. ARBs don’t affect bradykinin, so cough happens in only 3-5% of users. That’s why ARBs are often the go-to alternative when someone can’t tolerate an ACE inhibitor.
Why Combining Them Is Risky
You might think: if one drug lowers blood pressure, two must be better. That’s a logical assumption-but it’s wrong here. Multiple large studies have shown that combining ACE inhibitors and ARBs doesn’t give you better survival rates, fewer heart attacks, or slower kidney decline. What it does give you is a much higher chance of serious side effects.
The ONTARGET trial in 2008 followed over 25,000 high-risk patients. Half got ramipril (an ACE inhibitor), half got telmisartan (an ARB), and half got both. The combination group had no improvement in heart attacks, strokes, or death. But their risk of needing dialysis jumped from 1% to 2.3%. Hyperkalemia-dangerously high potassium-rose from 2.5% to 5.5%. That’s more than double.
Other studies, like the VA NEPHRON-D trial in 2018, confirmed this pattern. In diabetic patients with kidney disease, adding an ARB to an ACE inhibitor increased serious adverse events by 27% without protecting kidney function. The FDA and major medical societies now say: do not combine ACE inhibitors and ARBs outside of rare, tightly monitored cases.
When Cross-Reactivity Matters
Even switching from one class to the other isn’t risk-free. If you stop an ACE inhibitor and start an ARB right away, you’re not giving your body time to reset. The renin-angiotensin system can go into overdrive during the transition, causing a sudden drop in blood pressure or worsening kidney function.
Guidelines recommend a 4-week washout period between switching classes. But in practice, only about 4 in 10 doctors follow this. That’s dangerous. Patients who switch too quickly are more likely to end up in the ER with low blood pressure, dizziness, or acute kidney injury.
Also, if you’ve had angioedema (swelling of the face, tongue, or throat) on an ACE inhibitor, you’re at higher risk of getting it again on an ARB-even though the risk is lower. About 0.1-0.7% of ACE inhibitor users get angioedema. For ARBs, it’s 0.1-0.2%. Still, if you’ve had it once, most doctors will avoid ARBs entirely and choose a different class of blood pressure medication.
Who Might Still Get Both?
There’s a small group of patients where doctors might consider combining these drugs-but only as a last resort. These are people with non-diabetic kidney disease, like focal segmental glomerulosclerosis (FSGS), who still have protein loss in their urine (over 1 gram per day) despite being on the highest tolerated dose of an ACE inhibitor.
In these rare cases, adding an ARB might cut proteinuria by 25-40%. But it’s not a decision made lightly. Patients need weekly blood tests for potassium and kidney function. They’re watched like hawks. And even then, many doctors still avoid it.
One nephrologist at Massachusetts General Hospital reported discontinuing combination therapy in 87% of her patients with diabetic kidney disease because of rising potassium or dropping kidney function. That’s not an outlier. A 2023 survey of 317 primary care doctors found that only 11% still use the combination, and only with monthly lab checks.
What to Do Instead
If your blood pressure isn’t controlled on one RAS blocker, don’t reach for the other. There are safer, proven options.
- For extra blood pressure control: Add a low-dose thiazide diuretic like hydrochlorothiazide.
- For kidney protection with proteinuria: Add a mineralocorticoid receptor antagonist like spironolactone (12.5 mg daily). Studies show it cuts proteinuria by 30-40% with a better safety profile than ARB-ACE combos.
- For heart failure: Consider an ARNI (angiotensin receptor-neprilysin inhibitor), like sacubitril/valsartan. It’s been shown to outperform ACE inhibitors in survival and hospitalization rates.
These alternatives don’t carry the same risks. They’re backed by solid evidence. And they’re recommended in the 2023 ACC/AHA and ESC guidelines.
Monitoring Is Non-Negotiable
Even when you’re on just one of these drugs, you need regular blood tests. Both ACE inhibitors and ARBs can raise potassium and lower kidney function-especially in older adults, diabetics, or those with existing kidney disease.
Check your potassium and creatinine:
- 1-2 weeks after starting or changing the dose
- Every 3 months once you’re stable
If your potassium goes above 5.5 mmol/L or your creatinine rises more than 30% from baseline, your doctor needs to act. That’s not just a lab result-it’s a warning sign. Left unchecked, high potassium can cause dangerous heart rhythms. A sudden drop in kidney function could mean you’re at risk of needing dialysis.
People with diabetes, heart failure, or chronic kidney disease are at highest risk. But even healthy adults on long-term therapy can develop these issues over time. That’s why ongoing monitoring isn’t optional-it’s essential.
Real-World Problems
Behind the numbers are real people. On Reddit’s r/medicalschool, 78% of residents said they’ve seen a patient hospitalized for hyperkalemia after being put on both an ACE inhibitor and ARB. One 68-year-old man with diabetes was prescribed lisinopril and losartan together after his blood pressure didn’t drop. Two weeks later, he was in the ER with a potassium level of 6.8. He needed emergency treatment and spent five days in the hospital.
On the flip side, a few patients with rare kidney diseases have seen big improvements with combination therapy. But these are exceptions-not the rule. And they’re managed under strict supervision.
The takeaway? Don’t assume more drugs = better results. Sometimes, less is more.
What’s Next?
Research is still evolving. The FINE-REWIND trial, running from 2024 to 2028, is testing whether very low doses of both drugs might offer kidney protection without the usual risks. Results won’t be out until late 2026.
Meanwhile, the market is shifting. ACE inhibitors still dominate prescriptions-58% in the U.S. in 2023. But ARBs are catching up, especially because they’re better tolerated. And new drugs like ARNIs are replacing both in heart failure treatment.
One thing won’t change: the warning against combining ACE inhibitors and ARBs. The data is too clear. The risks are too high. The benefits? Nonexistent.
Can I take an ACE inhibitor and ARB together for better blood pressure control?
No. Combining ACE inhibitors and ARBs does not improve survival, heart attack rates, or long-term kidney outcomes. It doubles your risk of hyperkalemia and increases the chance of acute kidney injury by nearly twice. Major guidelines from the AHA, ACC, and ESC strongly advise against this combination except in rare, research-approved cases.
I had a cough from lisinopril. Is it safe to switch to losartan?
Yes. ARBs like losartan don’t cause the dry cough associated with ACE inhibitors because they don’t increase bradykinin. About 90% of people who can’t tolerate ACE inhibitors due to cough do well on ARBs. Still, wait at least 4 weeks after stopping the ACE inhibitor before starting the ARB to avoid sudden drops in blood pressure or kidney function.
How often should I get blood tests if I’m on an ACE inhibitor or ARB?
Get your potassium and creatinine checked 1-2 weeks after starting or changing the dose. Once stable, check every 3 months. If you have diabetes, kidney disease, or are over 65, your doctor may want checks every 2 months. High potassium or rising creatinine can signal serious problems that need quick action.
What are the signs of hyperkalemia from these drugs?
High potassium often has no symptoms at first. But as levels rise, you might feel muscle weakness, fatigue, irregular heartbeat, or nausea. In severe cases, it can cause cardiac arrest. That’s why regular blood tests are critical-don’t wait for symptoms. If you’re on an ACE inhibitor or ARB, assume your potassium could rise and get it checked regularly.
Are there safer alternatives to combining ACE inhibitors and ARBs?
Yes. For extra blood pressure control, add a low-dose diuretic like hydrochlorothiazide. For kidney protection with proteinuria, spironolactone (12.5 mg daily) is proven to reduce protein loss by 30-40% with fewer risks than combining ACE inhibitors and ARBs. For heart failure, ARNIs like sacubitril/valsartan have shown better outcomes than ACE inhibitors alone.
Can I switch from an ARB back to an ACE inhibitor safely?
Yes, but wait at least 4 weeks after stopping the ARB. Switching too quickly can cause a rebound effect in the renin-angiotensin system, leading to low blood pressure, dizziness, or kidney stress. Always consult your doctor before switching-never make the change on your own.





pradnya paramita
February 3, 2026 AT 22:08Combining ACEi and ARBs is a classic pharmacokinetic blunder-both agents suppress RAS at different nodes, leading to unopposed renin release and compensatory aldosterone surges. The resultant hyperkalemia and acute kidney injury aren't just statistical anomalies; they're predictable pharmacodynamic cascades. ONTARGET and VA NEPHRON-D aren't just trials-they're cautionary blueprints. The 2.3% dialysis rate in combo therapy? That's not risk-it's inevitability in high-risk cohorts.
Even in FSGS, the 25-40% proteinuria reduction doesn't justify the 5.5% hyperkalemia risk when spironolactone offers comparable efficacy with lower mortality. Guidelines aren't suggestions-they're the product of meta-analyses with 50k+ patient-years of data.
Zachary French
February 5, 2026 AT 09:10Y'ALL ARE OVERCOMPlicating THIS. ACE inhibitors cause cough? Yeah, because they make your throat feel like sandpaper. ARBs don't? Cool. But guess what? They still make your kidneys act up if you're not watchin' 'em. I had a cousin on both-doc said 'it'll help'-two weeks later he was in the ER with potassium so high his heart almost stopped. Like… why are we even still debating this? The data's been out since 2008. People just don't wanna admit they got lazy.
Daz Leonheart
February 7, 2026 AT 06:48Just want to say-this is the kind of post that makes me feel less alone in this. I’ve been on lisinopril for 7 years and switched to valsartan after the cough got unbearable. Took the full 4-week break like my nephrologist said. Felt weird at first-like I was floating-but my BP stabilized and my creatinine stayed put. No drama. No ER visits. Just quiet, consistent care. It’s not sexy, but it works.
And yeah, the diuretic trick? That’s what finally got my BP under control after years of chasing the perfect combo. HCTZ 12.5mg. Simple. Safe. Effective. Don’t overthink it.
Caleb Sutton
February 7, 2026 AT 13:15They don’t want you to know this, but the pharmaceutical industry pushes combo therapy because it’s more profitable. The FDA? They’re slow. The trials? Funded by the same companies that make the drugs. You think they’d tell you the truth? Look at the numbers-27% more adverse events and they still let it slide. Wake up. This isn’t medicine. It’s a business model.
Jamillah Rodriguez
February 8, 2026 AT 09:37Okay but like… why do doctors even *try* this combo? 😒 I had my grandma put on both and she spent a week in the hospital with ‘fluid overload.’ Like… did they not read the same textbook I did? Also, why is no one talking about how ARNIs are the real MVP now? 🙄
Susheel Sharma
February 8, 2026 AT 15:04The fundamental flaw in clinical practice is the assumption that pharmacological synergy implies clinical benefit. This is a reductionist fallacy. The RAS is not a linear pathway-it is a dynamic, feedback-rich network. Suppressing two nodes simultaneously induces compensatory upregulation of aldosterone, endothelin, and sympathetic tone, thereby negating any theoretical advantage. The data are unequivocal: no mortality benefit, only iatrogenic harm.
Spironolactone, at 12.5 mg, is not merely an alternative-it is a superior modulator of proteinuria in CKD, with a more favorable risk-benefit ratio than dual RAS blockade. The 2023 ESC guidelines reflect this paradigm shift. Why are we still debating 2008 evidence in 2025?
Roshan Gudhe
February 9, 2026 AT 09:07It’s funny how we treat medicine like a menu-‘I’ll have the ACE, extra ARB, and hold the guidelines.’ But the body isn’t a restaurant. It’s an ecosystem. When you disrupt one part, everything else shifts. The RAS isn’t just a blood pressure dial-it’s tied to inflammation, fibrosis, even mental health. We’ve forgotten that healing isn’t about stacking drugs. It’s about listening-to the data, to the patient, to the body’s own wisdom.
That 4-week washout? It’s not bureaucracy. It’s respect. Respect for the system that’s been working for millions of years before we ever invented pills.
And yeah, ARNIs? They’re the future. Not because they’re new, but because they don’t just block-they rebalance. That’s the difference between control and harmony.
Jesse Naidoo
February 9, 2026 AT 16:18So you’re telling me I can’t just double down on my meds to get my BP lower? That’s literally the opposite of everything I’ve been taught since med school. I’m gonna need a minute.
Samuel Bradway
February 11, 2026 AT 07:44My dad’s on lisinopril. He checks his potassium every 3 months like clockwork. No drama. Just routine. This post saved his life-I showed it to his doctor and they finally stopped trying to add another pill. Sometimes less really is more.