Gallbladder and Biliary Disease: Understanding Stones, Cholangitis, and ERCP

When your gallbladder stops working right, the pain doesn’t just come and go-it hits like a wave you can’t swim out of. Imagine a sharp, steady ache under your right ribs that lasts for hours, maybe even days. You might feel nauseous, feverish, or notice your skin turning yellow. These aren’t random symptoms. They’re your body screaming about gallstones, infected bile ducts, or a blockage that needs immediate attention. Gallbladder and biliary diseases affect over 20 million Americans, with women more than twice as likely to be affected as men. And while many people live with silent gallstones, others face life-threatening complications that demand quick, precise care.
What Are Gallstones, and Why Do They Form?
Gallstones are hardened deposits of bile, the fluid your liver makes to help digest fat. They form when something’s out of balance in your bile. About 80% are made mostly of cholesterol, often when your liver dumps too much into your gallbladder and it crystallizes. The other 20% are pigment stones, made from bilirubin, a waste product from broken-down red blood cells. These are more common in people with liver disease, sickle cell anemia, or those of Asian descent.Size matters. Some stones are tiny, like grains of sand. Others grow as big as golf balls. Most people never know they have them-about 80% of gallstones are asymptomatic. But when one gets stuck, trouble follows. If it blocks the cystic duct (the tube connecting your gallbladder to the bile duct), you get acute cholecystitis: inflammation, swelling, fever, and severe pain. If it moves into the common bile duct, you risk cholangitis-a dangerous infection-or pancreatitis, where digestive enzymes start digesting your own pancreas.
Who’s at risk? Obesity, rapid weight loss, diabetes, and being over 60 all raise your odds. Women are more prone due to estrogen’s effect on bile composition. Native American populations, especially Pima Indians, have the highest rates globally-up to 64% in some groups. If you’ve had bariatric surgery or are on birth control, your risk goes up too.
Cholangitis: When the Bile Ducts Get Infected
Cholangitis isn’t just discomfort-it’s a medical emergency. It happens when a stone or tumor blocks the common bile duct, trapping bacteria that normally flow harmlessly out of the liver. The infection builds, and your body reacts hard. The classic signs, called Charcot’s triad, show up in most cases: severe pain in the upper right abdomen, fever, and jaundice (yellow skin or eyes). If you add low blood pressure or confusion, you’ve reached Reynolds’ pentad. That means septic shock is near.Without treatment, cholangitis can kill. Studies show mortality rates jump to over 20% if it’s not treated within 24 hours. That’s why doctors don’t wait. If you have these symptoms, you need imaging and antibiotics fast. The go-to test? MRCP-magnetic resonance cholangiopancreatography. It’s non-invasive, has 95% accuracy for spotting bile duct stones, and doesn’t expose you to radiation. It’s the first step before anything else.
But MRCP only shows the problem. It doesn’t fix it. That’s where ERCP comes in.
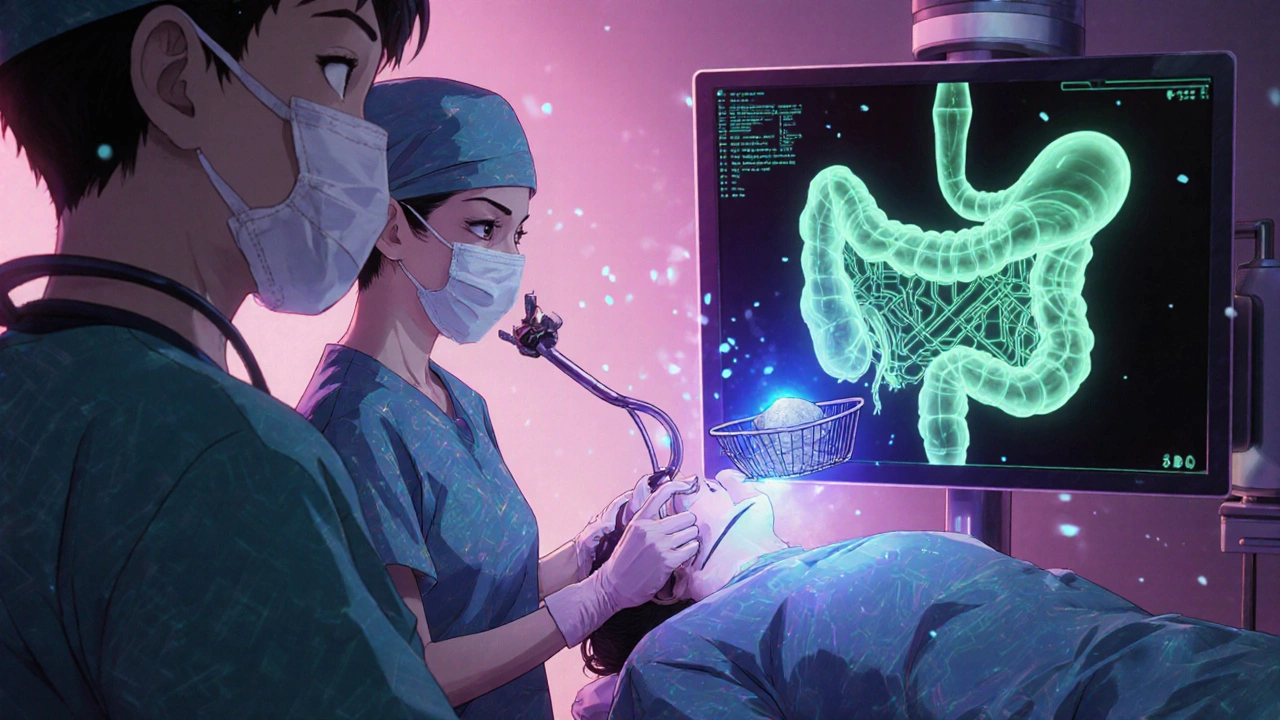
ERCP: The Procedure That Fixes Blocked Bile Ducts
Endoscopic Retrograde Cholangiopancreatography (ERCP) is a hybrid procedure-part endoscopy, part X-ray. A thin, flexible tube with a camera is threaded through your mouth, down your esophagus, into your stomach, and into the first part of your small intestine. There, the doctor finds the opening where the bile duct and pancreatic duct meet-the ampulla of Vater. A tiny catheter is passed through the scope, dye is injected, and X-rays show exactly where the stone is stuck.Then comes the fix. The doctor uses a tiny wire or basket to pull the stone out, or cuts the muscle around the duct opening (sphincterotomy) to let it pass. In some cases, a stent is placed to keep the duct open. The whole thing takes 30 to 90 minutes. Most people go home the same day.
Success rates? Over 90% in experienced hands. But it’s not risk-free. About 3-10% of patients develop post-ERCP pancreatitis, which can be mild or severe. That’s why doctors don’t use ERCP just to look. The American College of Gastroenterology says: “Use MRCP first. Only do ERCP if you’re going to treat.” Still, when it’s needed, it’s often the only way to avoid major surgery.
There’s a big gap in care: only 30-40% of patients with bile duct stones get their stones removed during the same procedure as their gallbladder removal. That means hundreds of thousands of people end up with two separate hospital visits, two sets of anesthesia, and two recovery periods. Better coordination between surgeons and endoscopists could cut that down.
What Happens After Gallbladder Removal?
If your gallbladder is removed (cholecystectomy), you don’t need it to live. Your liver keeps making bile-it just flows straight into your small intestine instead of being stored. Most people feel better right away. One study found 87% of patients had major symptom relief within 30 days after surgery.But not everyone. About 12% develop post-cholecystectomy syndrome: ongoing pain, bloating, or diarrhea. Why? Sometimes the original diagnosis was wrong. Sometimes bile flows too fast, irritating the intestine. Other times, tiny stones were missed or the sphincter of Oddi (a valve at the end of the bile duct) becomes dysfunctional.
After surgery, most doctors recommend a low-fat diet for 2-4 weeks. Your body needs time to adjust. Many people can return to normal eating within six weeks. But some struggle with loose stools long-term. If you’re one of them, over-the-counter medications like loperamide can help. Talk to your doctor-it’s more common than you think.
What Doesn’t Work Anymore
You might have heard about pills to dissolve gallstones. Ursodeoxycholic acid (UDCA) can work-but only for small cholesterol stones (under 15mm) and only about 30-40% of the time. It takes 6 to 12 months. And it doesn’t touch pigment stones. Plus, stones often come back after you stop taking the drug.Shock wave therapy (lithotripsy) was once tried to break stones apart. But it’s rarely used now. Why? It doesn’t work well on multiple stones, and over half the people who get it develop new stones within five years. It’s not worth the cost or hassle.
And don’t rely on “natural remedies.” Apple cider vinegar, lemon juice, or gallbladder flushes won’t dissolve stones. At best, they’re harmless distractions. At worst, they delay real treatment.

What’s New in 2025
Technology is catching up. In 2023, the FDA approved a new type of duodenoscope-one with a fully disposable elevator mechanism. Before, these scopes were linked to deadly outbreaks of drug-resistant infections because they’re hard to clean. Now, the risky parts are thrown away after each use.Another advance? Intraductal ultrasonography (IDUS). This tiny ultrasound probe goes inside the bile duct during ERCP. It can spot stones smaller than 5mm that standard X-rays miss. That’s huge for people with unexplained pain and normal MRCP results.
Researchers are also hunting for new drugs to dissolve pigment stones, which currently have no effective medical treatment. That could change everything for people with liver disease or sickle cell.
And telehealth is helping. Post-ERCP check-ins over video reduce hospital readmissions by 18% in pilot programs. You don’t need to drive across town for a follow-up if your symptoms are stable.
When to See a Doctor
Don’t wait for a crisis. If you have:- Severe, lasting pain under your right rib cage
- Fever with chills and jaundice
- Nausea and vomiting that won’t go away
- Dark urine or pale stools
-get checked. Start with an ultrasound. If that shows stones and you’re symptomatic, you’ll likely need surgery. If your doctor suspects a stone in the bile duct, they’ll order an MRCP. If it confirms a blockage, ERCP is next.
And if you have gallstones but no symptoms? Don’t rush to surgery. The risk of complications from silent stones is only 1-2% per year. The risks of surgery often outweigh that. Watch and wait, unless you’re in a high-risk group-like someone with a polyp in the gallbladder or a history of pancreatitis.
Final Thoughts
Gallbladder and biliary disease isn’t a one-size-fits-all problem. It’s a spectrum-from silent stones to life-threatening infections. The good news? We have tools to handle almost every stage. Ultrasound, MRCP, ERCP, and laparoscopic surgery are precise, safe, and effective when used correctly.The biggest mistake? Delaying care or chasing unproven fixes. The second biggest? Getting surgery when you don’t need it. If you’re unsure, get a second opinion. Ask your doctor: “Is this stone causing my symptoms, or am I being treated for something I might never have problems with?”
Most people who get the right care at the right time go back to their lives-no more midnight pain, no more fear of the next attack. And that’s the real goal: not just removing a gallbladder, but removing the burden of disease.



Latrisha M.
November 16, 2025 AT 17:32My mom had silent gallstones for years until she woke up with jaundice and a fever. ERCP saved her life. No drama, no miracle cures, just a smart doctor who knew when to act. If you’re reading this and have symptoms, don’t wait for it to get worse.
Jamie Watts
November 17, 2025 AT 06:36Ursodeoxycholic acid is a joke and everyone knows it. I’ve seen 3 patients waste 8 months on that crap only to end up in surgery anyway. And don’t even get me started on lemon juice cleanses. People are so gullible. MRCP then ERCP if needed. End of story. Stop listening to TikTok healers.
Rachel Wusowicz
November 18, 2025 AT 22:14Did you know the FDA approved those disposable duodenoscopes only after 17 people died from superbugs in one hospital in 2018? They knew. They knew the scopes were impossible to sterilize properly-and still let them be used for years. Now they’re ‘fixed’? Maybe. Or maybe they just stopped reporting the outbreaks. Who’s really behind this? Pharma? The device manufacturers? The same people who told us asbestos was safe.
Diane Tomaszewski
November 20, 2025 AT 16:48It’s wild how something so simple-like a gallbladder-can cause so much chaos. I used to think it was just a fancy storage tank. Turns out it’s more like a pressure valve that can explode if you ignore it too long. And the fact that most people never know they have stones until it hits them… it’s like your body’s whispering until it screams.
Oyejobi Olufemi
November 21, 2025 AT 08:59You think this is about medicine? No. This is about control. The system wants you dependent. Gallstones? They could be dissolved with natural minerals. But why sell you a $15,000 ERCP when you can buy a $5 supplement? Hospitals make billions from fear. They don’t want you to know that fasting and magnesium can dissolve stones. They want you scared, on the table, and paying. This is medical colonization.
Daniel Stewart
November 21, 2025 AT 23:52There’s a quiet tragedy in how we treat chronic illness-reducing complex physiological signals to binary decisions: remove it or don’t. But what if the body isn’t broken? What if it’s trying to tell us something? Maybe the gallbladder isn’t the enemy-it’s the messenger. And we’ve spent centuries punishing messengers instead of listening.
John Mwalwala
November 23, 2025 AT 19:13Here’s the real kicker: the sphincter of Oddi dysfunction is massively underdiagnosed. Most docs think it’s IBS or anxiety. But if you’ve had cholecystectomy and still get biliary-type pain? Get an ERCP with manometry. The pressure readings are the key. Most gastroenterologists don’t even know how to order it. That’s why 12% of post-op patients are stuck in limbo. It’s not incompetence-it’s systemic ignorance.
Deepak Mishra
November 25, 2025 AT 11:44OMG I JUST HAD THIS!!! 😭 I thought it was food poisoning but then my eyes turned yellow and I cried for 3 hours. ERCP was scary but like… 10/10 would do again if needed. My doc was a godsend. Also, I drank apple cider vinegar for a week before and it did NOTHING. Don’t be me. Go to the hospital. 💪🩺
Dan Angles
November 26, 2025 AT 18:06It is imperative to underscore the importance of interdisciplinary coordination between surgical and endoscopic teams. The current fragmentation of care, wherein patients undergo separate procedures for cholecystectomy and common bile duct stone removal, represents a significant inefficiency in resource utilization and patient morbidity. Standardized protocols, including intraoperative cholangiography and same-admission ERCP, are not merely optimal-they are ethically warranted.
David Rooksby
November 28, 2025 AT 07:42So let me get this straight-you’re telling me the same people who told us smoking was fine in the 50s are now telling us ERCP is the gold standard? And we’re supposed to trust them? I’ve seen too many people get post-ERCP pancreatitis and then get told it’s just a ‘known risk.’ What about the risk of being misdiagnosed because MRCP missed a 3mm stone? What about the fact that 60% of bile duct stones are missed on ultrasound? This whole system is built on assumptions, not evidence. And now they’re selling us disposable scopes like it’s a victory? It’s a Band-Aid on a bullet wound.
Melanie Taylor
November 30, 2025 AT 05:06As a Nigerian-American, I’m so glad this post mentioned pigment stones and sickle cell. My cousin had them and no one in the U.S. knew to test for it. We had to go back to Lagos for a specialist. Please, if you’re Black, Indigenous, or Asian-know your risk. Don’t wait for symptoms to be ‘typical.’ We don’t always fit the textbook.
Teresa Smith
December 1, 2025 AT 09:40There’s a reason we don’t remove asymptomatic gallstones. The risks of surgery-bleeding, infection, bile leak-are real. And the chance of a silent stone ever causing trouble? Less than 2% per year. That’s lower than the risk of dying in a car crash on your way to the hospital for a ‘preventive’ surgery. Don’t let fear drive your decisions. Get informed. Get a second opinion. And if your doctor pushes surgery without clear symptoms? Walk out. You’re not broken. You’re just living with a quirk your body adapted to.