Mycosis Fungoides Types: Complete Guide to Diagnosis & Treatment

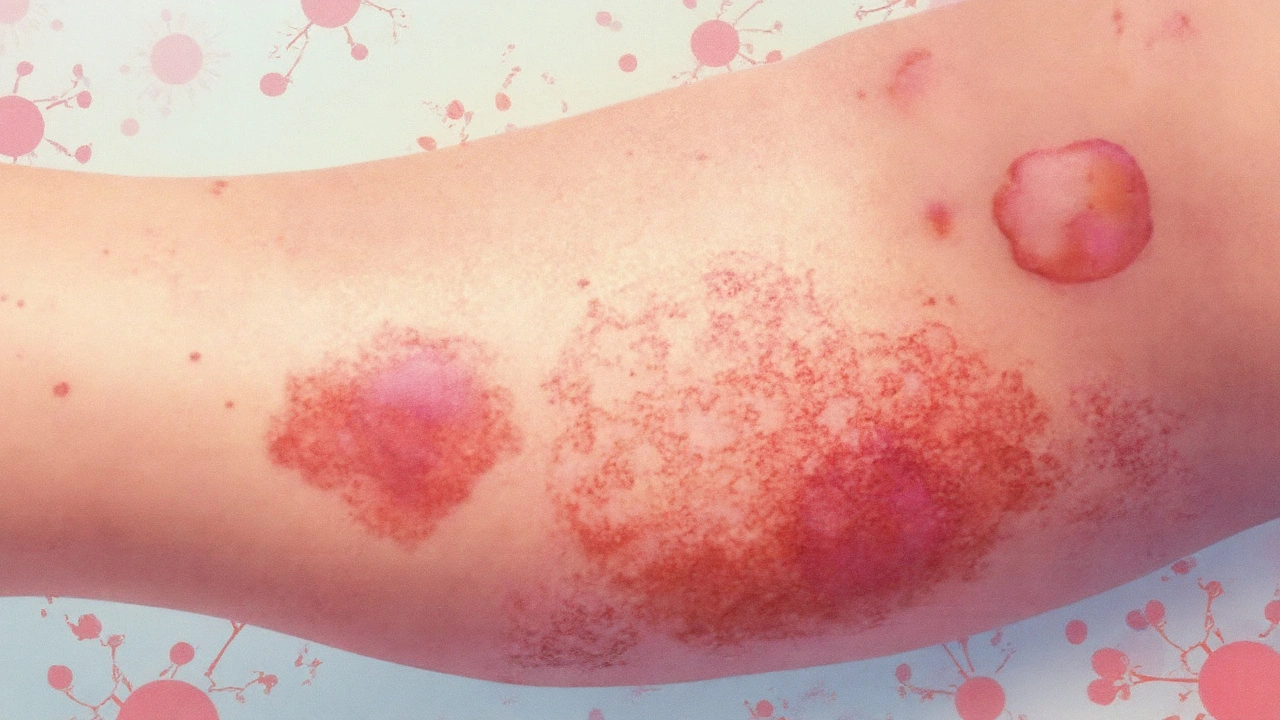
Mycosis Fungoides is a rare, slow‑growing cutaneous T‑cell lymphoma that typically begins as scaly patches and can evolve into plaques or tumors. It represents the most common form of primary skin‑based lymphoma, accounting for about 50% of cases worldwide. Because the disease can masquerade as eczema or psoriasis, recognizing its distinct variants is critical for early intervention.
Why a Separate Look at the Variants Matters
Each subtype carries its own clinical pattern, prognosis, and preferred treatment. Misidentifying a follicular or granulomatous form as classic Mycosis Fungoides can delay therapy and affect survival. This guide walks you through the five most frequently encountered types, how they are diagnosed, and what patients can expect.
Quick Reference (TL;DR)
- Classic MF: patches → plaques → tumours; indolent; skin‑directed therapy works early.
- Folliculotropic MF: follicle‑centered lesions, often alopecic; deeper infiltration, tougher to treat.
- Pagetoid Reticulosis: solitary, slowly expanding plaque; excellent prognosis with local therapy.
- Granulomatous MF: granuloma‑like nodules; may mimic infections; systemic therapy often needed.
- Sézary syndrome: leukemic counterpart; widespread erythroderma, poorer outlook.
Clinical Spectrum of Mycosis Fungoides
The disease is not a single picture; it ranges from flat, barely visible patches to nodular tumours that ulcerate. Below is a high‑level view of how the variants differ in presentation, typical age of onset, and response to treatment.
| Type | Typical Skin Appearance | Average Age at Diagnosis | Prognosis (5‑yr survival) | First‑Line Treatment |
|---|---|---|---|---|
| Classic Mycosis Fungoides | Patch → Plaque → Tumour | 55‑65years | ≈90% | Topical steroids, phototherapy |
| Folliculotropic MF | Follicular papules, alopecia, deep plaques | 45‑60years | ≈70% | Retinoids, total skin electron beam |
| Pagetoid Reticulosis | Solitary, well‑demarcated plaque | 30‑50years | ≈95% | Local radiotherapy or excision |
| Granulomatous MF | Nodular granuloma‑like lesions | 50‑70years | ≈80% | Systemic retinoids, interferon‑α |
| Sézary Syndrome | Erythroderma, circulating malignant T‑cells | 60‑70years | ≈30‑40% | Extracorporeal photopheresis, systemic therapy |
Deep Dive: Each Variant Explained
Classic Mycosis Fungoides
Classic MF begins with flat, erythematous patches that often look like eczema. Over years, these patches thicken into plaques and may eventually develop tumours. Histology shows epidermotropism-atypical CD4⁺ T‑cells infiltrating the epidermis. Immunohistochemistry typically reveals loss of CD7 and over‑expression of CD30 in transformed lesions.
Folliculotropic Mycosis Fungoides (FMF)
FMF targets hair follicles, producing follicular papules, cyst‑like nodules, and often localized alopecia. Because the malignant cells sit deeper, routine skin biopsies can miss the diagnosis; a deeper incisional biopsy is recommended. Studies from the International Society for Cutaneous Lymphoma (2023) show a median overall survival of 7years, shorter than classic MF.
Pagetoid Reticulosis (PR)
Also called “Woringer‑Kolopp disease,” PR presents as a single, slowly enlarging plaque usually on the extremities. The lesion contains intraepidermal atypical lymphocytes that spread in a pagetoid pattern-hence the name. Treatment is straightforward: local radiotherapy (8‑12Gy) or surgical excision yields cure rates above 95%.
Granulomatous Mycosis Fungoides
Granulomatous MF generates nodules that histologically resemble sarcoidosis or infectious granulomas. Special stains for acid‑fast bacilli and fungi are negative, helping to rule out infection. Systemic agents such as bexarotene or low‑dose methotrexate are commonly employed, with response rates around 60% in recent clinical series.
Sézary Syndrome (SS)
Though technically a leukemic variant of cutaneous T‑cell lymphoma, SS shares many molecular features with MF (e.g., high CD4/CD7 loss). Patients experience generalized redness, itching, and circulating Sézary cells detectable by flow cytometry. Management leans heavily on extracorporeal photopheresis combined with systemic agents like romidepsin.
Diagnostic Work‑up Across the Spectrum
Accurate classification hinges on clinicopathologic correlation. The typical workflow includes:
- Full‑body skin exam and photographic documentation.
- Punch or incisional biopsy targeting the most representative lesion.
- Histopathology with H&E staining plus immunophenotyping for CD3, CD4, CD7, CD30.
- Blood work: CBC, LDH, Sézary cell count (if erythroderma present).
- Imaging (CT or PET) when tumour‑stage disease is suspected.
Emerging molecular tools-T‑cell receptor (TCR) gene rearrangement studies and next‑generation sequencing-help confirm clonality, especially in early‑stage disease.
Treatment Strategies Tailored to Each Type
Therapy follows a stage‑guided algorithm, but the variant informs drug choice.
- Early‑stage classic MF: Topical corticosteroids, nitrogen‑mustard, or UV‑B phototherapy.
- Folliculotropic MF: Systemic retinoids (bexarotene) plus total skin electron beam (TSEB) for extensive disease.
- Pagetoid Reticulosis: Local radiotherapy or surgical excision; systemic therapy rarely needed.
- Granulomatous MF: Interferon‑α or low‑dose methotrexate; consider biologics if refractory.
- Sézary Syndrome: Extracorporeal photopheresis with HDAC inhibitors or alemtuzumab.
All patients benefit from skin‑care education-gentle moisturizers, avoidance of irritants, and regular follow‑up.
Prognosis & Follow‑Up Considerations
Overall 5‑year survival exceeds 85% for early‑stage classic MF, but drops dramatically for tumour‑stage disease and Sézary syndrome. Regular monitoring every 3‑6months includes skin exams, blood counts, and imaging when indicated. Early detection of transformation (e.g., CD30‑positive large‑cell transformation) prompts escalation to multi‑agent chemotherapy.
Related Conditions and How They Differ
Understanding the boundaries helps avoid misdiagnosis.
- Cutaneous T‑cell Lymphoma (CTCL): Umbrella term that includes MF, SS, and rare entities like primary cutaneous CD30‑positive lymphoproliferative disorder.
- CD30‑positive lymphoproliferative disorder: Presents with solitary or clustered nodules; responds well to topical brentuximab.
- Langerhans cell histiocytosis: Skin lesions may mimic MF plaques but show CD1a⁺, langerin⁺ cells on immunostain.
- Psoriasis: Well‑demarcated plaques with silvery scale; lacks atypical epidermotropic lymphocytes.
When a clinician is unsure, a multidisciplinary tumor board-dermatology, pathology, oncology-usually settles the diagnosis.
Next Steps for Patients and Providers
After reading this guide, the logical actions are:
- Schedule a full‑body skin examination if you notice persistent patches or nodules.
- Ask your dermatologist about a biopsy that reaches the deep dermis, especially for suspected FMF.
- If diagnosed, discuss the stage‑specific treatment plan and consider enrolling in a clinical trial (many are open for novel agents like mogamulizumab).
- Implement a skin‑care regimen to reduce irritation and improve quality of life.
- Set up a follow‑up schedule-typically every 4‑6weeks for the first year.
Staying informed and proactive can shift the odds toward a favorable outcome.
Frequently Asked Questions
What is the earliest sign of Mycosis Fungoides?
The first clue is often a flat, red, scaly patch that does not respond to standard eczema creams. If the patch persists for more than six months, a skin biopsy is warranted.
How does Folliculotropic MF differ from classic MF?
Folliculotropic MF attacks hair follicles, causing follicular papules, cysts, and localized hair loss. The malignant cells sit deeper in the skin, so a superficial punch biopsy may miss them, requiring a deeper incisional sample.
Is Pagetoid Reticulosis curable?
Yes. Because it usually appears as a single plaque, localized treatments like excision or low‑dose radiotherapy cure >95% of patients.
What systemic therapies are used for advanced Mycosis Fungoides?
Options include bexarotene, interferon‑α, low‑dose methotrexate, histone deacetylase inhibitors (e.g., vorinostat), and monoclonal antibodies such as brentuximab vedotin for CD30‑positive disease.
How is Sézary syndrome diagnosed?
Diagnosis requires three criteria: (1) erythroderma covering >80% of body surface, (2) circulating Sézary cells (≥1000 cells/µL) with aberrant immunophenotype, and (3) clonally rearranged T‑cell receptor genes.
Diagnosis requires three criteria: (1) erythroderma covering >80% of body surface, (2) circulating Sézary cells (≥1000 cells/µL) with aberrant immunophenotype, and (3) clonally rearranged T‑cell receptor genes.



anthony perry
September 24, 2025 AT 08:01Got a patch that won't go away? Get it biopsied. Simple.
Cole Brown
September 26, 2025 AT 04:01This is super helpful. I’ve seen so many people misdiagnosed with eczema for years. If you’ve got a rash that doesn’t respond to cream, don’t just keep trying new lotions. See a derm. Seriously.
Amy Craine
September 28, 2025 AT 00:36Classic MF is often misread because it looks like psoriasis or dermatitis-but the epidermotropism is the key. T-cell receptor clonality testing should be standard in ambiguous cases, especially if the lesion persists beyond six months. Early detection changes outcomes.
LeAnn Raschke
September 29, 2025 AT 22:42Thank you for writing this. I’m a nurse and I’ve seen patients suffer because no one took their ‘rash’ seriously. This guide is clear, practical, and gives hope. Please share it with every dermatology office.
Craig Venn
September 30, 2025 AT 18:10FMF is a sneaky one. Superficial biopsies miss it every time. You need deep punch or incisional. I’ve had cases where patients were on steroids for 2 years before we realized it was folliculotropic. The hair loss is a huge red flag. Also, bexarotene + TSEB works better than people think.
Alicia Buchter
October 1, 2025 AT 21:12Ugh. Another ‘medical authority’ dumping jargon. Who even reads this? If you’re not a dermatologist, this is just noise. Why not just say ‘if it doesn’t heal, get a biopsy’? Why the whole damn textbook?
MaKayla VanMeter
October 2, 2025 AT 03:20OMG I’ve had this for 7 years and no one believed me 😭😭😭 I thought I was going crazy. They called it ‘stress rash’ and gave me hydrocortisone. Now I know it’s MF. Thank you for validating me 💕
Danny Pohflepp
October 2, 2025 AT 04:23Let’s be real-this is all a Big Pharma ploy. The real cause of Mycosis Fungoides is glyphosate exposure in genetically susceptible populations. The FDA suppresses data linking environmental toxins to cutaneous lymphomas. Why are there no studies on soil contamination? Why is phototherapy the ‘gold standard’? Coincidence?
Halona Patrick Shaw
October 3, 2025 AT 04:20Yo. I’m from the South and we’ve got a cousin who had Pagetoid Reticulosis. Doc said ‘it’s just a weird rash’ for two years. Then he did a biopsy, did a 10-minute radiation, and boom-gone. Like it never happened. That’s the miracle right there. Don’t sleep on local treatment.
Suresh Patil
October 4, 2025 AT 17:47In India, many patients delay care because they think skin rashes are normal. This guide should be translated. Granulomatous MF is often mistaken for tuberculosis here. We need more awareness. Thank you for the clarity.
Ram Babu S
October 5, 2025 AT 11:24My uncle had Sézary. It was brutal. The itching was worse than the redness. ECP helped him breathe easier. If you’re reading this and you’re newly diagnosed-hang in there. Progress is slow but real. We’ve seen miracles.
Kyle Buck
October 6, 2025 AT 17:25The TCR clonality data is critical for early-stage diagnosis, particularly in patch-phase disease where histopathology is equivocal. The sensitivity of NGS-based assays has improved significantly since 2020, with >92% concordance with flow cytometry in recent cohorts. This should be integrated into diagnostic algorithms before systemic therapy is initiated.
Sarah Major
October 8, 2025 AT 14:12People are so naive. You think this is just a ‘rash’? This is cancer. And you’re probably reading this because you’ve been ignoring it for years. You’re lucky it’s not metastasized yet. Stop scrolling and go see a doctor.
Amber Walker
October 10, 2025 AT 12:40I just got diagnosed with classic MF and I’m terrified but this guide made me feel less alone. Thank you. I’m starting phototherapy next week. Praying it works 💪
Adorable William
October 10, 2025 AT 23:10Interesting how the ‘standard’ treatments all involve radiation or synthetic retinoids. But no one talks about the fact that vitamin D3 analogs have shown comparable efficacy in murine models with zero toxicity. Why are we still using toxic systemic agents when nature provides alternatives? This feels like institutional inertia disguised as science.
Elizabeth Nikole
October 11, 2025 AT 18:34You’re all so dramatic. It’s just skin. You act like you’re dying. I’ve had eczema my whole life and I’m fine. Maybe you’re just anxious. Stop Googling. Go outside. Breathe. It’s not cancer. Probably.