Lisinopril and Pregnancy: Risks, FAQs, and Safe Alternatives

When you’re pregnant and need to control blood pressure, Lisinopril is a drug you’ll hear a lot about - but not for the right reasons. Lisinopril and pregnancy is a hot topic because this medication belongs to a class that can cross the placenta and harm a developing baby. Below we break down what you need to know, how to spot trouble, and which safer options are available.
What Is Lisinopril and How Does It Work?
Lisinopril is an ACE inhibitor (angiotensin‑ converting enzyme inhibitor). It relaxes blood vessels by blocking the conversion of angiotensin I to angiotensin II, a powerful vasoconstrictor. The result: lower blood pressure and reduced strain on the heart.
For most adults with hypertension or heart failure, lisinopril is a first‑line choice because it’s once‑daily, inexpensive, and well studied. However, the same mechanism that helps adults can be dangerous for a fetus.
Why Lisinopril Is a Concern During Pregnancy
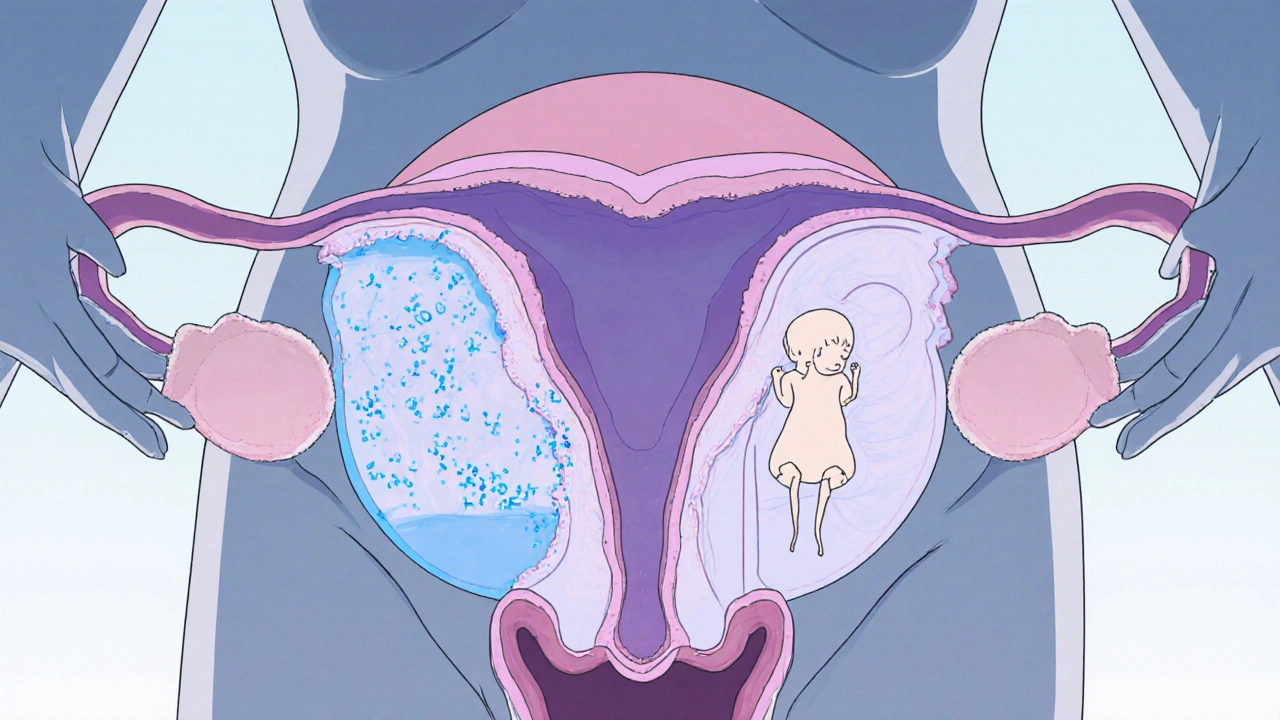
During pregnancy, the renin‑angiotensin system (RAS) plays a critical role in fetal kidney development and blood‑flow regulation. ACE inhibitors interfere with this system, potentially leading to:
- Fetal renal agenesis or dysplasia (under‑developed kidneys)
- Oligohydramnios - too little amniotic fluid, which can compress the fetus
- Pulmonary hypoplasia (under‑developed lungs)
- Growth restriction and even fetal demise in severe cases
Because these risks become more pronounced after the first trimester, most guidelines advise stopping ACE inhibitors as soon as pregnancy is confirmed.
Regulatory Stance: FDA and Professional Guidelines
The FDA categorizes lisinopril as Pregnancy Category D - meaning there is positive evidence of risk, but the drug may be used if the potential benefits outweigh the risks. The American College of Obstetricians and Gynecologists (ACOG) recommends switching to safer antihypertensives as soon as pregnancy is detected.
What the Risks Look Like in Real Life
Case reports from the early 2000s showed clusters of newborns with severe renal abnormalities after maternal exposure to ACE inhibitors in the second or third trimester. A 2022 meta‑analysis of 13 studies (over 2,000 pregnancies) found a 4‑fold increase in oligohydramnios and a 2.5‑fold rise in fetal kidney malformations when ACE inhibitors were continued beyond 12 weeks.
Most of the data come from retrospective reviews, but the signal is clear enough that clinicians treat lisinopril as contraindicated after the first trimester.
How to Know If You’ve Been Exposed
- Confirm the timing - any dose after conception, especially after 8‑12 weeks, raises concern.
- Watch for reduced fetal movement or abnormal ultrasound findings (e.g., low amniotic fluid).
- Ask your obstetrician for a detailed fetal anatomy scan between 18‑22 weeks.
- If exposure was early (first trimester), the risk of major malformations is lower, but follow‑up imaging is still advised.
Never stop lisinopril on your own; abrupt withdrawal can cause rebound hypertension, which is also dangerous for mother and baby.
Safer Blood‑Pressure Medications in Pregnancy
Several antihypertensives have robust safety data and are recommended by both the FDA and ACOG:
| Medication | Drug Class | FDA Pregnancy Category | Typical Use |
|---|---|---|---|
| Labetalol | Beta‑blocker + Alpha‑blocker | Category C (generally safe) | First‑line for mild‑moderate hypertension |
| Methyldopa | Central alpha‑agonist | Category B | Long‑standing safety record, used in chronic hypertension |
| Nifedipine (extended‑release) | Calcium‑channel blocker | Category C | Effective for acute severe hypertension |
| Hydralazine | Direct vasodilator | Category C | Often used in severe cases or pre‑eclampsia |
Among these, Labetalol is frequently the go‑to because it controls both systolic and diastolic pressure without compromising uterine blood flow.
Managing Hypertension After Stopping Lisinopril
If you’re already on lisinopril and discover you’re pregnant, the typical pathway is:
- Immediate consultation with your obstetrician and primary care provider.
- Gradual tapering of lisinopril over 2‑3 days to avoid rebound spikes.
- Initiation of a pregnancy‑safe alternative (often labetalol).
- Regular blood‑pressure monitoring - home cuff readings at least twice daily.
- Follow‑up labs to watch kidney function and electrolytes.
Close collaboration between your cardiologist, obstetrician, and pharmacist ensures a smooth transition.
Key Takeaways Checklist
- Never take Lisinopril after confirming pregnancy.
- If you become pregnant while on lisinopril, contact your doctor right away.
- Switch to a pregnancy‑safe antihypertensive such as labetalol, methyldopa, or extended‑release nifedipine.
- Schedule a detailed fetal anatomy scan between 18‑22 weeks.
- Monitor blood pressure daily and keep a log for your care team.
Frequently Asked Questions
Can a single early‑trimester dose of lisinopril cause birth defects?
The risk is much lower in the first trimester, but it’s not zero. Most experts still recommend a thorough ultrasound and consider switching to a safer drug as soon as possible.
What symptoms might indicate fetal kidney problems?
Reduced amniotic fluid (oligohydramnios) on ultrasound is the most common sign. It may be accompanied by a smaller‑than‑expected fetal bladder or absent kidney shadows.
Is it safe to restart lisinopril after delivery?
Yes, once you’re no longer breastfeeding and your doctor confirms your kidney function is normal, lisinopril can be restarted if it’s the best option for you.
How do I manage blood pressure if I’m allergic to labetalol?
Methyldopa or extended‑release nifedipine are solid alternatives. Your provider can tailor the dose based on your baseline pressures.
Will my insurance cover the switch to a pregnancy‑safe drug?
Most plans cover generic labetalol and methyldopa. If a brand product is needed, ask your pharmacist about prior‑authorization options.
Pregnancy is a time when every medication decision matters. Knowing the risks of lisinopril, acting quickly, and partnering with knowledgeable clinicians puts you and your baby on the safest possible path.



Lionel du Plessis
October 25, 2025 AT 16:20ACEi cross placenta – monitor renal markers
Andrae Powel
October 26, 2025 AT 18:33First off, I’m really sorry you’re navigating this-it’s stressful but you’re not alone. The key is to get on a pregnancy‑safe antihypertensive like labetalol or methyldopa as soon as you confirm your pregnancy. Talk to your OB‑GYN and ask for a detailed anatomy scan around 20 weeks; that’ll catch any renal abnormalities early. Keep a blood pressure log and share it with your care team so they can adjust doses promptly. If you ever feel a sudden spike, don’t wait-call your provider. It’s also a good idea to have your pharmacist review any other meds you’re on, because drug interactions can sneak up on you. Remember, abrupt stopping of lisinopril can cause rebound hypertension, so a gradual taper is essential. You’ll feel more in control when you have a clear plan, and most women end up having healthy pregnancies once the switch is made. Hang in there, and keep the lines of communication open with your doctors.
Jennie Smith
October 27, 2025 AT 23:43Oh wow, thanks for laying this all out! 🎉 It’s such a relief to finally see a clear checklist-never thought I’d be reading about “renal agenesis” in a casual scroll. The table of alternatives is gold; I’ve already bookmarked labetalol as my go‑to. The way you broke down the timing of risk (especially after 12 weeks) really helps me visualise my own timeline. I can already picture the ultrasound at 20 weeks, hoping for a full‑sized bladder on the screen. Also, kudos for mentioning the importance of not stopping lisinopril cold-my sister learned the hard way. This post feels like a lifeline for anyone scrambling for answers mid‑pregnancy. Keep the awesome content coming!
Greg Galivan
October 29, 2025 AT 02:56Lisinopril is a dangerous drug in pregnancy its risks are real stop it as soon as possible you cant risk fetal kidney problems
Anurag Ranjan
October 29, 2025 AT 03:13Agreed – immediate taper and switch to labetalol is the safest route.
James Doyle
October 30, 2025 AT 05:53The pharmacodynamic profile of lisinopril, while advantageous in the management of systemic hypertension, becomes a liability once the gestational environment introduces a delicate balance of vasoactive mediators. Its irreversible inhibition of angiotensin‑converting enzyme disrupts the renin‑angiotensin axis that is essential for fetal nephrogenesis. Consequently, the downstream cascade leads to oligohydramnios, a surrogate marker for compromised renal output. Clinical registries have consistently reported a four‑fold increase in adverse renal outcomes when exposure extends beyond the first trimester. Moreover, the teratogenic signal is not limited to renal structures; pulmonary hypoplasia has been documented secondary to reduced amniotic fluid volume. From a hemodynamic perspective, abrupt discontinuation of lisinopril without a tapering protocol can precipitate rebound hypertension, which in itself poses a risk of placental insufficiency. Thus, the therapeutic transition must be orchestrated with a multidisciplinary team, incorporating obstetrics, cardiology, and pharmacy expertise. Labetalol, with its combined α‑ and β‑adrenergic blockade, offers a favorable safety profile that preserves uteroplacental perfusion. Methyldopa, though older, remains a viable option owing to its central sympatholytic mechanism and extensive pregnancy data. Extended‑release nifedipine provides rapid vasodilation for acute spikes and is categorized as FDA Class C, which is acceptable when benefits outweigh potential risks. Hydralazine is reserved for severe cases such as pre‑eclampsia, where direct arteriolar relaxation is required. Patient education should emphasize the importance of home blood pressure monitoring, ideally twice daily, to capture any rebound trends. Serial ultrasounds between 18 and 22 weeks are indispensable for assessing amniotic fluid volume and fetal kidney morphology. Laboratory surveillance of serum creatinine and electrolytes should continue throughout the transition phase. In the postpartum period, once lactation ceases and maternal renal function stabilizes, lisinopril can be reinstated if it remains the optimal agent. Overall, the guiding principle is to minimize fetal exposure while maintaining maternal cardiovascular stability.
Edward Brown
October 31, 2025 AT 09:40One might wonder why the mainstream medical establishment pushes ACE inhibitors so aggressively then pulls the rug when pregnancy enters the equation – is it a matter of profit, or is there a deeper orchestration at play? The fact that the FDA still lists it as Category D despite clear teratogenic signals feels like a deliberate obfuscation; perhaps the data is being suppressed. If you think about the renin‑angiotensin system as a tightly regulated network, tampering with it during gestation is akin to hacking a critical infrastructure while the city is under construction. It raises the question: who benefits from the continued prescription of a drug that endangers fetal development? The answer may lie beyond the scope of conventional obstetrics, hidden in the corridors of pharmaceutical lobbying.
ALBERT HENDERSHOT JR.
October 31, 2025 AT 09:56Your concerns are understandable, and it’s important to stay critical of the information sources we rely on. However, the consensus guidelines are based on extensive clinical data that have consistently demonstrated the risks of ACE inhibitors in pregnancy. Switching to labetalol or methyldopa has been shown to maintain maternal blood pressure control while protecting fetal development. Let’s keep the focus on evidence‑based practice 😊.
Suzanne Carawan
November 1, 2025 AT 13:26Oh great, another reminder that we can’t trust any medication once we’re pregnant. Because apparently the universe decided that a simple blood pressure pill should turn into a murder weapon. Thanks for the panic.
Kala Rani
November 2, 2025 AT 17:13And yet some still claim lisinopril is safe late in pregnancy