Rifampin Induction: How It Lowers Anticoagulant and Antiviral Levels
Rifampin Interaction Risk Calculator
Select Medication
Risk Assessment
When you’re on rifampin for tuberculosis or to prevent meningitis, you might not think twice about your other medications-until something goes wrong. A patient on warfarin for a mechanical heart valve starts rifampin, and suddenly their INR drops from 2.8 to 1.1. No bleeding, no clots-yet. But the risk is there. That’s not a rare mistake. It’s a predictable, well-documented drug interaction that happens every day in clinics across the U.S., and it’s often missed because the signs aren’t dramatic until it’s too late.
How Rifampin Changes How Your Body Processes Drugs
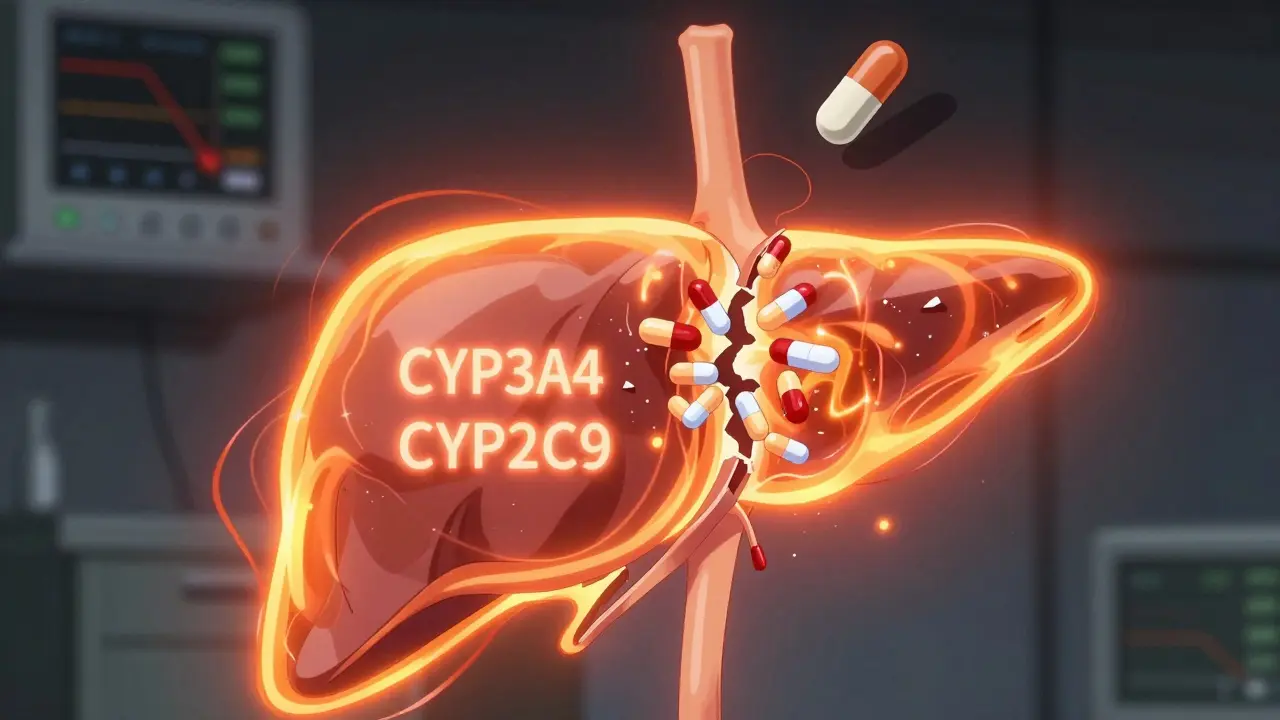
Rifampin doesn’t just kill bacteria. It rewires your liver. It activates something called the pregnane X receptor, or PXR. This isn’t a drug target you hear about often, but it’s the reason rifampin is one of the most powerful drug-interaction agents in medicine. When PXR turns on, it tells your liver to make more of certain enzymes-mainly CYP3A4 and CYP2C9. These enzymes are like trash compactors for drugs. They break down medications so your body can get rid of them faster.
The result? Drugs that used to last 12 hours now last 4. That’s why your anticoagulant stops working. It’s not that rifampin cancels it out. It’s that your body burns through it before it can do its job. This effect starts within 24 to 48 hours after taking rifampin. By day 5 or 7, it’s at full power. And here’s the kicker: even after you stop rifampin, it takes 2 to 3 weeks for those enzymes to break down and go back to normal. So if you think stopping rifampin fixes the problem right away, you’re wrong.
Warfarin and Rifampin: A Dangerous Mix
Warfarin is the oldest oral anticoagulant, and it’s still widely used-especially in patients with mechanical heart valves or certain types of atrial fibrillation. But warfarin is a precision tool. Too little, and you get a stroke. Too much, and you bleed internally. Its narrow window makes it especially vulnerable to rifampin.
Studies show rifampin can slash warfarin levels by 15% to 74%. That’s not a range-it’s a warning. The S-isomer of warfarin, the more potent part, is broken down by CYP2C9, which rifampin strongly induces. One case report described a 57-year-old woman with a mechanical aortic valve. Her INR stayed stable on phenprocoumon (a warfarin-like drug) for years. After starting rifampin for suspected endocarditis, her INR dropped to normal levels within days. She had no symptoms. No warning. Just a silent loss of protection. It took 15 days after stopping rifampin for her INR to return to therapeutic levels.
Doctors used to think you could just increase the warfarin dose. But it’s not that simple. You might need three to five times the original dose to keep INR in range. Even then, it’s unstable. Small changes in diet, other medications, or even hydration can throw it off. The American College of Chest Physicians says the safest move? Switch to low molecular weight heparin injections during rifampin treatment. It’s not ideal-shots every day-but it’s predictable. No enzyme interference. No guessing.
DOACs Don’t Escape Either
Direct oral anticoagulants (DOACs) like apixaban, rivaroxaban, dabigatran, and edoxaban were supposed to be the easier, safer alternative to warfarin. No monthly blood tests. Fewer food interactions. But they’re not immune to rifampin. In fact, they’re just as vulnerable-just in different ways.
Rivaroxaban and apixaban are metabolized mostly by CYP3A4. When rifampin kicks in, their blood levels drop by 50% to 67%. That’s not a minor reduction. That’s the difference between protection and danger. Dabigatran, which is cleared partly through the kidneys and partly by P-glycoprotein (another transporter rifampin induces), also sees a 50%+ drop in concentration. Edoxaban drops about 35%, but its active metabolites rise, which might offer some protection-but not enough to rely on.
The European Heart Rhythm Association says it plainly: don’t combine DOACs with rifampin. The FDA’s own guidelines classify rifampin as a strong inducer that can reduce drug exposure by more than 80% in sensitive cases. And DOACs are sensitive. Unlike warfarin, there’s no easy way to check if they’re working. No INR test. No quick lab result. You’re flying blind.
One 2021 study in Frontiers in Pharmacology followed six patients with prosthetic joint infections who needed both rifampin and rivaroxaban. The researchers found that even with dose increases, the anticoagulant effect remained unpredictable. They recommended avoiding the combo unless there’s no other option-and even then, only with daily monitoring and expert oversight.
What About Antivirals?
Rifampin doesn’t just mess with blood thinners. It also wrecks antivirals. HIV medications like darunavir, rilpivirine, and elvitegravir are all broken down by CYP3A4. When rifampin is added, their levels can crash by 70% or more. That’s not just a risk of treatment failure-it’s a risk of drug resistance. A single missed dose of antiviral can let the virus mutate. And once it does, your treatment options shrink.
Hepatitis C drugs like sofosbuvir and daclatasvir are also affected. Even newer antivirals like nirmatrelvir (part of Paxlovid) are contraindicated with rifampin. The FDA label for Paxlovid explicitly says: Do not co-administer with strong CYP3A inducers like rifampin. That’s not a suggestion. That’s a hard stop.
For patients with HIV or hepatitis who need tuberculosis treatment, the challenge is real. Many end up delaying TB therapy to avoid losing control of their viral infection. Others switch to injectable TB drugs like amikacin or linezolid-less convenient, more side effects, but safer with antivirals.
What Should You Do?
If you’re on anticoagulants or antivirals and your doctor says you need rifampin, here’s what actually works:
- Don’t assume your current dose is enough. Even if you’ve been stable for years, rifampin changes everything.
- Switch to injectables if possible. For anticoagulation, low molecular weight heparin (like enoxaparin) is the gold standard during rifampin use. For antivirals, consult an infectious disease specialist-there are alternative TB regimens that don’t include rifampin.
- Monitor closely. If you must stay on warfarin, check INR every 2-3 days during the first two weeks of rifampin. Use a home monitor if you have one-accuracy is within ±0.5 INR units of lab tests.
- Don’t restart anticoagulants too soon. After stopping rifampin, wait at least 14 days before returning to your old dose. Reintroduce slowly and recheck levels.
- Ask about alternatives. Is there a non-rifampin TB regimen? Is there a different antiviral that won’t interact? These conversations save lives.
There’s one emerging hope: new anticoagulants like milvexian, which targets factor XIa instead of thrombin or factor Xa, appear to be less affected by CYP3A4 induction. Early studies suggest they may be safer with rifampin. But they’re not yet widely available. Until then, the old rules still apply.

Why This Keeps Happening
Here’s the uncomfortable truth: this interaction isn’t rare because doctors are careless. It’s rare because most aren’t trained to think about it. A 2022 survey found only 12% of U.S. hospitals have formal protocols for managing rifampin-DOAC interactions. Most rely on pharmacy alerts, which often get ignored or overridden. And when a patient is admitted for pneumonia and found to have TB, rifampin gets added fast. The anticoagulant? Often forgotten.
It’s also getting harder to avoid. Between 2010 and 2020, the percentage of patients on DOACs instead of warfarin jumped from 15% to 85%. That’s progress-until you realize most DOACs are more vulnerable to rifampin than warfarin. We traded one problem for a more invisible one.
What’s Next?
The FDA now requires all new drugs to be tested against strong inducers like rifampin before approval. That’s good. But it doesn’t help the millions already on these drugs. What we need is better education-not just for doctors, but for patients. If you’re on warfarin, apixaban, or any antiviral, and you’re prescribed rifampin, ask: What’s the plan if this interaction happens? Don’t wait for the INR to drop. Don’t wait for a clot to form. Ask now.
This isn’t about avoiding rifampin. It’s about using it safely. Tuberculosis kills. So do blood clots and uncontrolled viruses. The goal isn’t to choose one over the other. It’s to manage both without losing either.
Can I just increase my warfarin dose if I’m on rifampin?
You might need to, but it’s risky. Rifampin makes warfarin levels unpredictable. Even with a higher dose, your INR can swing wildly due to diet, illness, or other medications. The safest approach is switching to injectable anticoagulants like enoxaparin during rifampin treatment. If you must stay on warfarin, check your INR every 2-3 days and adjust under close medical supervision.
Are DOACs safer than warfarin when taking rifampin?
No. DOACs like apixaban, rivaroxaban, and dabigatran are just as affected by rifampin-sometimes more. Their levels drop by 50-67%, and unlike warfarin, there’s no easy way to monitor their effect. European guidelines recommend avoiding DOACs entirely with rifampin. If there’s no alternative, expert supervision and daily monitoring are essential.
How long does rifampin affect my medications after I stop taking it?
The enzyme-inducing effects last 2 to 3 weeks after you stop rifampin. Your liver needs time to break down the extra CYP3A4 and CYP2C9 enzymes. That’s why you can’t just stop rifampin and immediately go back to your old anticoagulant dose. Wait at least 14 days, then restart slowly with close monitoring.
Can I take rifampin with Paxlovid or other antivirals?
No. The FDA explicitly warns against combining rifampin with Paxlovid (nirmatrelvir/ritonavir) and several other antivirals. Rifampin can reduce antiviral levels by more than 70%, leading to treatment failure and drug resistance. If you need both, your doctor must switch you to a non-rifampin TB regimen or delay antiviral treatment.
Is there a blood test to check if rifampin is affecting my anticoagulant?
Only for warfarin-via the INR test. For DOACs like apixaban or rivaroxaban, there’s no routine blood test. Specialized labs can measure drug levels, but they’re expensive, slow, and not widely available. If you’re on a DOAC and rifampin, you’re relying on clinical judgment, not lab data.
What if I can’t switch from rifampin? Are there any anticoagulants that work with it?
Currently, no oral anticoagulant is truly safe with rifampin. Injectable heparins (like enoxaparin) are the only reliable option. Newer drugs like milvexian (a factor XIa inhibitor) show promise in early studies because they’re not metabolized by CYP enzymes, but they’re not yet approved for general use. Until then, avoid oral anticoagulants with rifampin unless under expert care.
Final Thought
Rifampin is a lifesaver for tuberculosis. But it’s also a silent saboteur of other treatments. The real danger isn’t the drug itself-it’s the assumption that because it’s been used for decades, everyone knows how to handle it. They don’t. And that’s why this interaction keeps causing harm. If you’re taking anticoagulants or antivirals, don’t wait for a problem to happen. Talk to your doctor before rifampin starts. Ask for a plan. Your life might depend on it.




Emma Addison Thomas
January 6, 2026 AT 18:39Just had to switch my mom from warfarin to enoxaparin when she started rifampin for TB. She’s 72, had a mechanical valve, and we almost missed it. No warning signs, just a weird fatigue. Home INR monitor showed 1.0. Scary stuff. I wish more docs talked about this upfront.
Mina Murray
January 8, 2026 AT 05:58Of course the FDA doesn’t warn people. Big Pharma doesn’t want you to know that DOACs are basically useless with rifampin. They made them expensive so you’d forget to check your levels. And now you’re paying for it with a stroke. This is why I only use warfarin and test every day. No magic pills. Just vigilance.
Christine Joy Chicano
January 9, 2026 AT 10:41What fascinates me is how rifampin hijacks the pregnane X receptor like a rogue system admin. It’s not just enzyme induction-it’s a full-scale genomic reprogramming. CYP3A4 and CYP2C9 aren’t just ‘trash compactors’-they’re phase I metabolic gatekeepers. The fact that this effect lingers for weeks after discontinuation suggests epigenetic memory in hepatocytes. We’re not just dealing with pharmacokinetics here. We’re dealing with transcriptional sabotage. And yet, most clinicians still treat it like a dosage tweak problem. It’s terrifying how underappreciated this is.
Adam Gainski
January 10, 2026 AT 13:16Good breakdown. I’ve seen this in my clinic too-patients on rivaroxaban for AFib, start rifampin for latent TB, and suddenly they’re back in with DVT. We switched them to Lovenox immediately. No debate. Also, the 2-3 week washout period is critical. One guy restarted apixaban after 5 days and ended up in the ER with a pulmonary embolus. Don’t guess. Test. Wait. Consult.
Anastasia Novak
January 11, 2026 AT 00:53Oh my god. I just realized my cousin took rifampin while on Eliquis and didn’t tell anyone. She’s lucky she didn’t die. This is why I hate medicine. Everyone’s so focused on the new shiny drugs they forget the basics. DOACs aren’t magic. They’re fragile. And rifampin is a chemical grenade. Why aren’t we screaming about this in every ER?
Paul Mason
January 11, 2026 AT 12:49Man, I got prescribed rifampin last year for a sinus infection (yeah, dumb doc). I was on warfarin and didn’t know any of this. My INR dropped to 1.2. I felt fine. Turned out I had a tiny clot in my leg. Took three weeks to fix. Don’t be like me. Ask questions. Even if you think you’re fine.
Katrina Morris
January 12, 2026 AT 17:02i never knew rifampin did this to meds 😅 i thought it was just for tb. my aunt is on dabigatran and just started rifampin-should i tell her? she’s kinda stubborn…
steve rumsford
January 14, 2026 AT 03:51so like… if you’re on Paxlovid and get TB, you just gotta wait? no way to do both? that’s wild. i’d rather get the virus than the shots.
Andrew N
January 15, 2026 AT 02:57It’s not that hard. Rifampin induces CYP3A4. DOACs are substrates. Warfarin’s S-isomer is CYP2C9. Basic pharmacology. If you didn’t know this, you shouldn’t be prescribing or taking these meds without consulting a pharmacist.
LALITA KUDIYA
January 16, 2026 AT 16:54in india we dont have much access to enoxaparin… so we just increase warfarin dose and check INR every 2 days. its not perfect but its what we have. god bless home monitors 🙏
Poppy Newman
January 17, 2026 AT 13:53Just read this whole thing. 🤯 So many people are at risk and don’t even know it. I’m sharing this with my nurse friend. We need a poster in every clinic. This deserves a viral thread.
Anthony Capunong
January 17, 2026 AT 23:11Why are we letting foreign TB protocols dictate U.S. anticoagulant care? We’ve got better drugs now. Why not just ban rifampin? It’s 2024. We can do better than 1960s medicine.