SSRI Antidepressants and Serotonin Syndrome Risk from Drug Interactions

What SSRIs Do and Why Interactions Matter
SSRIs are a class of antidepressants that increase serotonin levels in the brain by blocking its reabsorption. Common ones include sertraline (Zoloft), escitalopram (Lexapro), fluoxetine (Prozac), and paroxetine (Paxil). They’re prescribed for depression, anxiety, and OCD - and used by about 1 in 8 U.S. adults. But while they’re safer than older antidepressants, they carry a hidden danger: serotonin syndrome.
Serotonin syndrome isn’t rare. It’s underdiagnosed, often mistaken for the flu, heatstroke, or anxiety. But when it hits, it can kill. The condition happens when too much serotonin builds up in your brain, usually because you’re mixing SSRIs with other drugs that also boost serotonin. It’s not about taking too much of one pill - it’s about what you take with that pill.
How Serotonin Syndrome Actually Happens
Your brain needs serotonin to regulate mood, sleep, and muscle control. SSRIs stop your nerve cells from sucking serotonin back in after it’s released, so more stays around. That’s good - until another drug does the same thing. Add a second serotonin booster, and the system overloads.
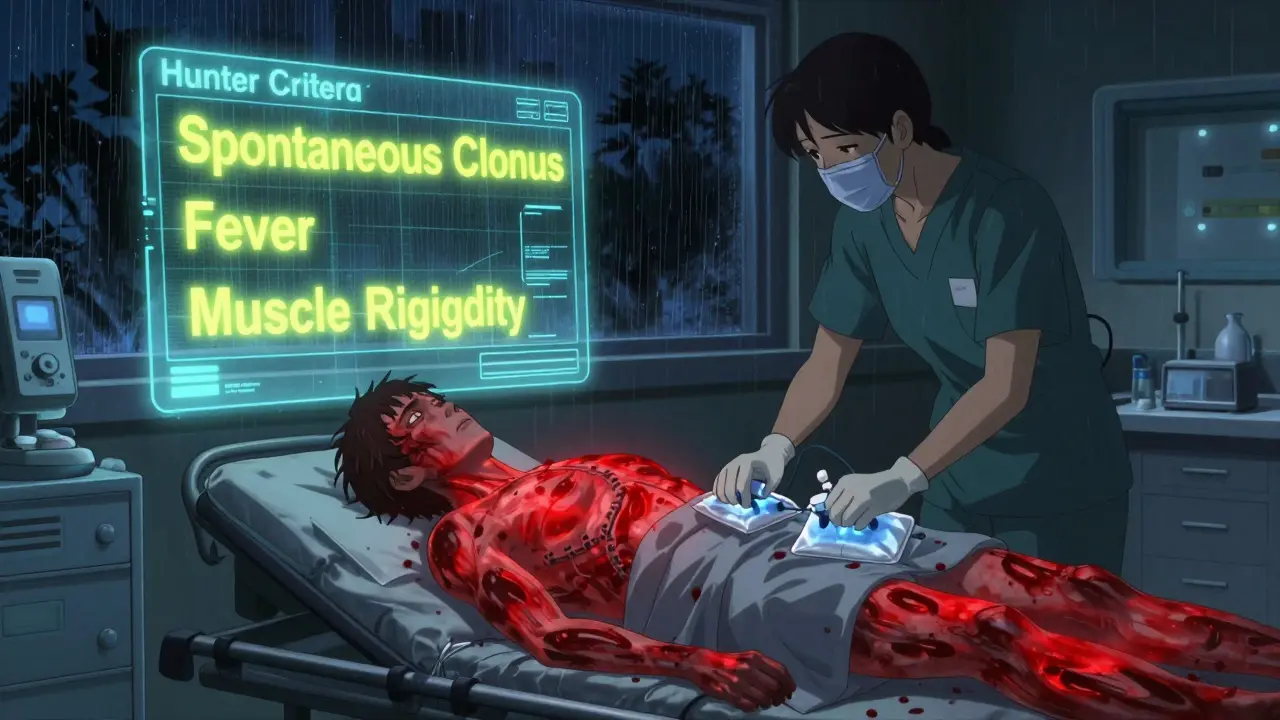
The symptoms come fast. You might feel agitated, start sweating heavily, or get muscle rigidity. Your body temperature can spike above 104°F. You could develop tremors, involuntary muscle contractions (clonus), or confusion. In severe cases, seizures, irregular heartbeat, or organ failure follow. The Hunter Serotonin Toxicity Criteria - the gold standard for diagnosis - says you need at least one of these: spontaneous clonus, inducible clonus with fever or sweating, or high muscle tone with fever and eye twitching.
Most cases happen within hours of adding a new drug. One Reddit user, on sertraline, took tramadol for back pain. Twelve hours later, he was in the ER with a 104.2°F fever and uncontrollable leg spasms. He spent three days hospitalized.
High-Risk Drug Combinations You Need to Know
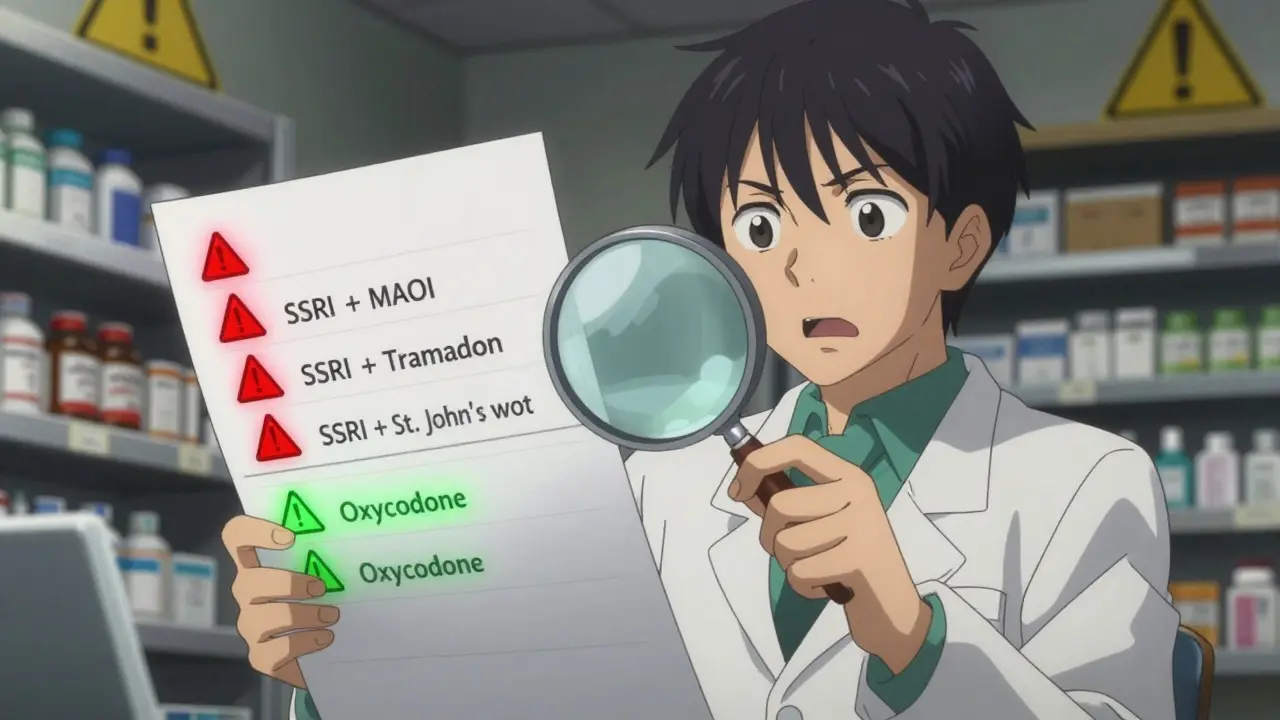
Not all drugs are equally dangerous when mixed with SSRIs. Some are red flags. Others are low risk. Here’s what actually matters:
- MAOIs - like phenelzine or selegiline - are the most dangerous. Combining them with SSRIs can be fatal. The mortality rate jumps to 30-50%. This combination is absolutely contraindicated.
- Linezolid - an antibiotic - has a 2.8 times higher risk of serotonin syndrome when taken with SSRIs. It’s not common, but if you’re on an SSRI and get prescribed linezolid, ask your doctor for an alternative.
- Tramadol, dextromethorphan, and pethidine - these opioids aren’t like morphine or oxycodone. They strongly boost serotonin. Tramadol, in particular, is a major culprit. A 2023 study found it increases serotonin syndrome risk by nearly five times when taken with SSRIs.
- SNRIs - like venlafaxine or duloxetine - are also antidepressants. Mixing them with SSRIs triples your risk. This happens often because doctors don’t realize both drugs are serotonergic.
- St. John’s wort - a popular herbal supplement - has been linked to serotonin syndrome in multiple case reports. One user on Drugs.com developed shivering and confusion after just three days of combining it with Prozac.
- Buspirone, tryptophan, and lithium - all increase serotonin. The FDA added them to its black box warning in 2006.
On the flip side, morphine, codeine, oxycodone, and buprenorphine show no significant risk increase. If you need pain relief while on an SSRI, these are safer choices.
Who’s Most at Risk?
It’s not just about what you take - it’s who you are.
- Older adults - 22% of Americans over 65 take five or more medications. Many are on SSRIs for depression and opioids for arthritis or back pain. This is the most common scenario for serotonin syndrome.
- People with CYP2D6 gene variations - about 7% of people are poor metabolizers of this liver enzyme. If you’re one of them and take tramadol with an SSRI, your risk is 2.4 times higher. Genetic testing isn’t routine, but if you’ve had bad reactions to meds before, ask about it.
- People recently starting or changing doses - the highest risk is in the first few days after adding a new drug or increasing an SSRI dose.
- Patients in hospitals - especially those getting antibiotics like linezolid or pain meds like tramadol. A 2022 JAMA study found 0.14% of elderly patients on SSRIs and linezolid developed serotonin syndrome. That sounds low, but in a hospital of 10,000, that’s 14 preventable cases.
What Doctors and Pharmacists Should Do
Healthcare providers have tools to prevent this.
- Washout periods - switching from an SSRI to an MAOI? Wait at least two weeks. For fluoxetine, wait five weeks because it sticks around so long.
- Electronic alerts - hospitals using Epic or Cerner now get pop-up warnings when an SSRI and tramadol are prescribed together. Since 2022, these alerts have cut dangerous combinations by 32% across 200 U.S. hospitals.
- Pharmacist reviews - a 2023 study showed pharmacist-led medication checks reduced serotonin syndrome events by 47% in Medicare patients. Ask your pharmacist to review all your meds - including supplements.
- Guidelines - the American Psychiatric Association and CDC now explicitly recommend avoiding tramadol, dextromethorphan, and pethidine in patients on SSRIs. They suggest oxycodone or morphine instead.
What You Can Do Right Now
If you’re on an SSRI, here’s your action plan:
- Make a list - write down every pill, patch, supplement, and herbal product you take. Include over-the-counter cough syrups (dextromethorphan), painkillers (tramadol), and even CBD oil (some brands affect serotonin).
- Ask your doctor - “Could any of my meds cause serotonin syndrome?” Don’t assume they know. Many don’t.
- Know the 5 S’s - Shivering, Sweating, Stiffness, Seizures (rare), Sudden confusion. If you develop any of these after starting a new drug, seek help immediately.
- Don’t stop your SSRI cold turkey - withdrawal can cause its own problems. Talk to your doctor before making any changes.
- Check your supplements - St. John’s wort, 5-HTP, and L-tryptophan are dangerous with SSRIs. Even some energy drinks with herbal stimulants can contribute.
What’s Changing in 2026
The system is catching up.
- The FDA now requires all electronic prescribing systems to show mandatory serotonin syndrome alerts for high-risk combinations. If your doctor tries to prescribe tramadol with sertraline, the system should block it or force a warning.
- A new blood test called SerotoninQuant is in late-stage trials at Mayo Clinic. By 2026, it could confirm serotonin syndrome objectively - no more guessing.
- Drug labels are being updated. All antidepressants now carry stronger warnings about opioid interactions.
But until those tools are everywhere, the responsibility falls on you. You’re the only one who knows every pill you take.
When to Go to the ER
Don’t wait. If you’re on an SSRI and you develop:
- High fever (above 102°F)
- Severe muscle stiffness or spasms
- Confusion, hallucinations, or agitation
- Fast heart rate or unstable blood pressure
- go to the ER immediately. Tell them you’re on an SSRI and recently started a new medication. Time matters. Early treatment with benzodiazepines and cooling can save your life.
Final Reality Check
SSRIs save lives. But they’re not harmless. Serotonin syndrome is preventable - but only if you know the risks. The numbers don’t lie: over 8,000 serious cases and 100+ deaths happen every year in the U.S. alone, mostly from drug interactions. Most of them are avoidable.
You don’t need to fear your medication. But you do need to be informed. Talk to your doctor. Review your list. Know the signs. Your life might depend on it.



jay patel
February 2, 2026 AT 05:48so i was on zoloft for my anxiety and my back doctor gave me tramadol because i hurt myself lifting a cooler of soda (yes, that’s a thing) and 12 hours later i was sweating like i’d run a marathon in a sauna and my legs were twitching like i was electrocuted. went to er, they knew instantly. they said if i’d waited another hour i might’ve had seizures. now i carry a card in my wallet that says ‘SSRI + TRAMADOL = BAD IDEA’ and i show it to every doctor. you think you’re safe until your body turns against you.
Ellie Norris
February 2, 2026 AT 15:22thank you for this. i’m a pharmacist in london and we’ve had 3 cases this year alone where people mixed st john’s wort with their ssri because ‘it’s natural’ - yeah, and arsenic is natural too. i always do a med review and ask about supplements. people think herbal = safe. it’s not. if it affects your brain chemistry, it’s a drug. period. also, dextromethorphan in cough syrup? yeah, that’s a silent killer. check the label. it’s in everything.
Brittany Marioni
February 4, 2026 AT 00:35please, everyone, make a list. write it down. on paper. keep it in your phone. put it in your wallet. tell your pharmacist. tell your doctor. tell your mom. tell your dog. if you’re on an ssri, you’re not just taking one thing - you’re playing russian roulette with your neurotransmitters. and no, your cousin’s friend’s yoga instructor’s essential oil blend isn’t ‘safe’ just because it smells like lavender. serotonin syndrome doesn’t care how zen you are. it just wants to fry your nervous system. don’t be the statistic.
Monica Slypig
February 4, 2026 AT 22:53of course americans die from this. you take 17 supplements, 8 prescriptions, and a handful of energy drinks before breakfast. you think your body is a vending machine you can just jam coins into until it spits out happiness. meanwhile, in europe, we take one pill if we need it, and we don’t mix it with herbal nonsense or over-the-counter cough syrup like it’s a smoothie. this isn’t a tragedy - it’s a cultural failure. stop treating your brain like a video game you can mod with random internet drops.
Becky M.
February 6, 2026 AT 15:50i’m a nurse in a geriatric unit and i see this all the time. grandpa on cymbalta for depression, grandpa on oxycodone for arthritis, grandpa on tramadol because the other one hurt his stomach, grandpa on st. john’s wort because his daughter said it’s ‘natural.’ then he starts shivering, gets confused, and we find out he’s been on all four for three weeks. we treat it with benzos and cooling - it works - but it’s so preventable. please, if you’re over 60 and on meds, sit down with your pharmacist. let them do the math. your life is worth the 15 minutes.
Eli Kiseop
February 8, 2026 AT 14:47what about cbd oil i heard some brands have serotonergic effects is that true or just hype
Sandeep Kumar
February 9, 2026 AT 11:30indians dont have this problem because we dont take ssris unless absolutely necessary and even then we dont mix with random painkillers. we have ayurveda and wisdom. america is a pharmacy with a mental health crisis. you want to fix serotonin syndrome? stop giving pills to everyone who feels sad for a week.
Gary Mitts
February 11, 2026 AT 09:15tramadol is the silent killer. i knew a guy who took it for a pulled muscle. died in his sleep. no one knew why. autopsy showed serotonin syndrome. his doctor didn’t even know he was on zoloft. check your meds. seriously. just check.
Brett MacDonald
February 12, 2026 AT 16:05we are all just chemical ghosts dancing on a wire of neurotransmitters. the body is a temple but also a battlefield. ssri is not a cure it is a ceasefire. and when you bring another soldier into the room with a different uniform and a different agenda - well. you get a civil war in your synapses. the real question is not what to avoid but whether we should be playing god with serotonin at all.
Hannah Gliane
February 14, 2026 AT 11:15if you're taking st. john's wort with an ssri you're not just dumb - you're a walking biohazard. 😡💀 you think you're being holistic? you're being a liability. your brain is not a smoothie bar. stop mixing supplements like you're making a cocktail at a frat party. you're not a trendsetter - you're a cautionary tale waiting to happen. get your act together.